
Research Article | DOI: https://doi.org/10.31579/2690-1919/161
1 VITROBIO Research Institute, ZAC de Lavaur, 63500 Issoire, France.
*Corresponding Author: Ravi Shrivastava, VITROBIO Research Institute, Issoire, France.
Citation: Remi Shrivastava, Margot Ennuyer, Ravi Shrivastava (2021). Instant Antibacterial and Anti-Inflammatory Osmotic Polymeric Film to Treat Sore Throat in Children. J Clinical Research and Reports, 7(4); DOI:10.31579/2690-1919/161
Copyright: © 2021 Ravi Shrivastava, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 April 2021 | Accepted: 20 April 2021 | Published: 26 April 2021
Keywords: pharyngitis; children; polymeric film; treatment; osmotic film; pro-inflammatory cytokine; virus glycoprotein; throat infection; paracetamol
Background: Pharyngitis, a common viral throat infection in children, involving inflammation, widespread local bacterial contamination and tissue destruction. When clinical signs appear, the disease already became multifactorial. In the absence of any multitarget treatment, we conceived a new generation of topical, osmotic, anti-inflammatory, throat surface cleaning polymeric film, capable of detaching and draining throat surface contaminants nearly instantly.
Material and methods: A glycerol and polymer containing osmotic film was prepared. Osmotic film attracts hypotonic liquid from the throat tissue, which detach and drain throat surface contaminants and create a favorable environment for cell growth and healing. Specific pro-inflammatory cytokine and virus glycoprotein binding polymers were incorporated in the film to suppress the inflammation. An observational, randomized, placebo-controlled study was performed after the approval of ethical committee on 30 children aged between (3-15), presenting symptoms of acute pharyngitis. After randomization, test product (n=20) and saline control (n=10) solutions were applied as 3-4 throat sprays 4-5 times / day for 15-days. Change in all the key pharyngitis symptom (difficulty swallowing, throat inflammation, irritation, redness, and bacterial deposit) were evaluated employing two-tailed Student’s test for followed by the post hoc Bonferroni’s test for comparisons of multiple groups
Results: Only a few specific polymers were able to bind with viral proteins and/or cytokines in adequate filmogen concentrations. Throat surface cleaning and cytokine neutralization strongly decrease all the pharyngitis symptoms and need for antibiotic therapy compared to controls (p<0.05 from day 3 onwards). No adverse effects were noted in any of the groups.
Conclusion: Clinical results showed excellent efficacy and safety of osmotically active polymeric film. Polymeric drugs may represent an excellent multitarget treatment approach to minimize the use of antibiotics and chemical drugs in the future.
Throat infection or pharyngitis, is one of the most common in children. Pharyngitis is defined as an infection and irritation of the pharynx or tonsils which causes swollen throat, difficulty in swallowing, throat irritation, inflammation, pain, fever, fatigue, and headache. Secondary signs may include runny nose, cough, itchy and watery eyes. In 80% of cases, the origin of the disease is viral, particularly rhinovirus, adenovirus, parainfluenza virus, coxsackievirus, coronavirus, and cytomegalovirus [1-3]. Initially, virus attacks a few cells, starts growing, causes cellular damage, and when the cells die, hundreds of free new viral particles are released on the throat surface. The disease is nearly asymptomatic up to this stage. These newly liberated virus particles now attach to new healthy cells, cause widespread tissue damage, open gaps in the intact mucosa barrier and trigger a strong immune reaction [4]. Tissue damage leads to the growth of opportunistic bacteria, particularly group A Streptococcus pyogenes (GAS), releasing Streptococcal pyrogenic exotoxins (SpeA, SpeC, SpeG to SpeM), superantigen A (SSA), and mitogenic exotoxin Z (SmeZ). They activate a large proportion of T-cell population, of which innate immune cells (monocytes, macrophages, dendritic cells, T cells, NK lymphocytes…) elicit an excessive uncoordinated release of proinflammatory cytokines such as TNF-α,IL-6, IL-10, and IL-12 on the throat surface [5,6]. When symptoms start appearing, the disease became already multifactorial involving viral growth, extensive throat mucosa damage, gaps on the throat mucosa allowing systemic entry of contaminants, abundant proinflammatory cytokines and growing microorganisms on the throat surface visible as whitish deposits. If the infection is suppressed rapidly, the immune system produces anti-inflammatory cytokines such as IL-4 to stop inflammation and provide a favorable environment for cell growth to repair cellular damage. Unfortunately, in most cases, natural defenses are not sufficient to suppress the pathogens and the release of proinflammatory cytokines continues, leading to chronic disease which may last a few weeks. Children being more fragile, suffer more than adults. Treating such a multifactorial disease compulsorily requires a multi-target treatment but in the absence of such medications, analgesics, anti-pyritic, antibiotics, and anesthetics constitute the first-line symptomatic remedies [7-9]. These drugs cannot be used simultaneously, results are not instant, they have no effect on repairing damaged throat mucosa, and they may induce side-effects and/or antibiotic resistance [10,11].
The aim of this study was to test the efficacy and safety of a multi-target, osmotic, non-irritant, and stable film which can be applied on the throat surface to remove all the contaminants including bacteria, viruses, and pro-inflammatory cytokines simultaneously. Cleaning the throat surface should help regenerate cells in a chemical free environment to reconstitute throat mucosa and its natural defense functions. The conception and efficacy of such a pharyngitis treatment for children is explained.
1. Selection of an osmotic base: The aim was to find a highly osmotic yet non-irritant filmogen base. After screening different natural and synthetic osmotic, non-cytotoxic, absorbent, and stable liquids, glycerol was selected as the most convenient filmogen base. Osmotic and mucosal irritant potentials were determined in in vitro cell culture models [12,13] and bovine corneal opacity test (BCOP), as described by Schrage et al [14]. The glycerol film was rendered thick and absorbent by adding small quantities of a few commonly used food-grade thickenings agents.
1.2. Glycerol-polymer binding to render glycerol film mechanically resistant to liquid flow: Mechanical resistance of glycerol film was enhanced by adding specific glycerol molecule binding inert polymers. As specific polymers are known to bind with selected macromolecules (H, OH binding) and specific proteins [15] we identified those polymers, which can bind with glycerol molecules to render the glycerol film stable. Glycerol binding polymeric structures were further tested to evaluate their specific protein binding potential.
1.3. Evaluation of pro-inflammatory cytokine binding potential of glycerol binding polymers:
Polymers, such as plant tannins, are very big molecules. After glycerol binding, many polymeric H and OH sites remain free [16].
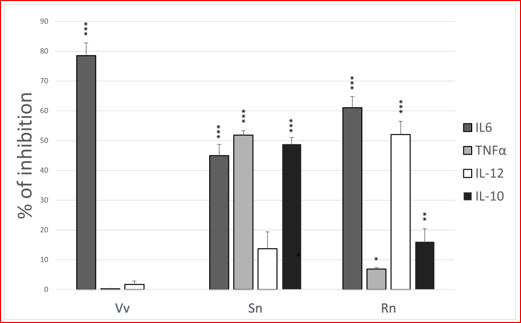
As tannin–protein binding is used to tan skin proteins and convert skin into leather, we used the same technology to evaluate polymeric affinity for pro-inflammatory cytokines. The polymeric binding affinity of the key child pharyngitis disease specific pro-inflammatory cytokines, such as TNF-α, IL-6, IL-10, and IL-12, was evaluated using ELISA tests at fixed polymeric concentration of 0.10% in 5.0% glycerol aqueous solution. Test products were incubated with each purified human recombinant cytokine (Invitrogen, 400 pg/ml) for 5 minutes in PBS. The remaining free and available recombinant cytokine was measured using Specific ELISA kit (Invitrogen, Human IL kits) according to the manufacturer's instructions. Recombinant cytokines without polymers were used as negative controls. The Optic Density (OD) was measured at 450 nm using an ELISA plate reader (luminometer-Envision, PerkinElmer).
Data analysis and interpretation: The scavenge activity of polymers is inversely proportional to the quantity of free cytokine detected. Reduction in quantified cytokine following incubation with polymers compared to the amount in negative controls, indicated the extent of cytokine neutralization due to polymeric binding.
2.0. Efficacy study: An observational efficacy trial was conducted at Mudra Clinical Research, India in 2019 (ISO-14155 certified clinical research organization, Registration N° SQ18N02, dated 05/09/2018, renewed up to 04/04/2021). The protocol and study design were approved by the Institutional Ashirwad Ethics Committee, India (Reg.No. ECR/247/Inst/MH/2013/RR-16, dated 07/08/2018). The study was conducted in accordance with the “Declaration of Helsinki”, concerning medical research in humans (Brazil, October 2013), and following the ICH-GCP guidelines. Informed consent was obtained from all children / parents involved in the study. All subjects gave their informed consent for inclusion before they participated in the study. Being an observational study with a Class I medical device used as a bandage for topical application, containing exclusively food grade ingredients and the evidence of safe use by above 100,000 children for this indication, CTR registration was not required.
Study design: The study was designed as an observational, comparative, randomized, parallel group to evaluate efficacy and safety of the test product (TP) compared to 0.9% saline solution sprays as comparator product (CP).
Key inclusion and exclusion criteria: Main inclusion criteria included (1) Boys and girls aged 3 to 15, (2) Having symptoms of recent throat infection (<72h), temperature >38°C, swelling of tonsils with >50% probability of positive culture for Streptococcus infection, (3) parents ready to provide written informed consent (4) Ready to abstain from other treatments except antibiotics in seriously ill patients to evaluate requirements of antibiotherapy. (5) Ready to follow the protocol and fill-up the daily questionnaire diary, (6) Not under any antiviral or anti-inflammatory treatment, (7) Not suffering from any chronic disease which may impact study parameters.
The main exclusion criteria were (1) Not meeting any of the above inclusion criteria, (2) Allergy to any of the investigational product ingredient, (3) Any disease or treatment which may affect study outcome.
Randomization: Treatments were allocated to patients by carrying out randomization using SAS Version 9.1.3. Biostatistician generated the randomization schedule. Block Randomization methodology was employed to follow 2:1 ratio in TP or CP groups.
Treatment: Test formulation contained an association of glycerol with dual acting glycerol + polymer binding association in water. CP contained 0.9% NaCl solution. The TP and CP were supplied as 30-ml sprays (about 100 sprays / vial, 3-4 sprays / application) to be applied on the throat surface every 20-30 minutes during the first 2h at the start of treatment and 3-4 times per day thereafter for a maximum period of 15-days.
Trial endpoints: Pharyngitis and/or throat infection related parameters were scored on a 1 to 7 scale (1=excellent; 7=worst). Key parameters recorded were: difficulty in swallowing, swollen throat, throat inflammation/redness, throat irritation, and presence of whitish microbial deposit on the throat surface. Throat swabs were examined at the start (Day 0) and at the end of the study. Number of days of antibiotic use in each group was also recorded. Mean scores of each symptom, at each time point, were compared with the baseline (BL: start of treatment) and between the groups on day 1 (2h after first treatment), day 3, day 7 and day 15 (end of the study).
Statistical analyses: Statistical analyses: The normality of the populations was determined by the Shapiro-Wilk test, then statistical analysis was performed by two-tailed Student’s test for comparisons between two groups and the two-way ANOVA followed by the post hoc Bonferroni’s test for comparisons of multiple groups. p<0.05 was considered statistically significant. The analyses were performed with the software GraphPad Prism (version 8.4.2, La Jolla, USA). NS indicates not significant.
Osmotic throat surface cleaning film: The polymer binding with glycerol formed a highly adherent and osmotic film, capable of generating a strong osmotic hypotonic liquid flow from the inner parts of the throat tissue. Polymeric binding with proinflammatory cytokines: To stabilize polymers and glycerol, only glycerol binding polymers were evaluated to identify those having affinity for selected cytokines. The aim was to find a polymeric association capable of binding with the four key proinflammatory cytokines involved in pharyngitis throat inflammation. Due avoid polymeric adherence in the solution, a unique 0.10% concentration of each polymer (n=18 each polymer) was screened in sandwich ELISA tests. Binding results revealed that polymer – protein binding is highly specific as only 10-15% polymeric structures had moderate to strong affinity for one or two cytokines. The Vv polymer derived from Vitis vinifera seeds, blocked nearly 78% IL-6 but had no effect on other cytokines. Sn polymer derived from Sambucus nigra fruit was capable to block nearly 45% IL-6 and nearly 50% TNF-alpha and IL-10 but had poor binding properties with IL-12. Rn polymer isolated from Ribes nigrum fruit extract, antagonized strongly IL-6 but was also capable of neutralizing above 50% IL-12. Therefore, these three polymers, having equally affinity for glycerol molecules, were used in concentrations between 0.10 to 0.40% to conceive the test product solution (Figure 1).
Finished formulation: The test product was specifically formulated (20-ml sprays) for throat application in children and contained glycerol (74.63%), a dual acting, glycerol and specific cytokine binding polymeric premix (0.83%), with excipients as described by Shrivastava et al [17].
Efficacy results: Among 34 children screened, 4 were dropped out before enrollment, 30 were randomized and all completed 15-day of scheduled treatment. The CP group was composed of
9 boys + 1 girl (mean age 7.9) while in the TP group, there were 7 boys + 13 girls (mean age 8.3).
Effect on swallowing difficulty

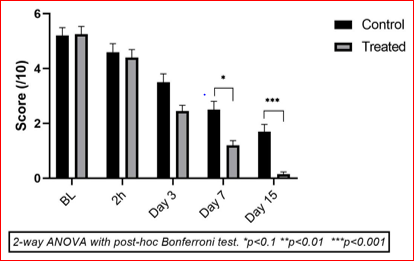
In figure 2, the scores were high in the saline (black bars, n=10) and polymeric spray treated (gray bars, n=20) groups at the start of treatment (baseline). Swallowing difficulties eased progressively during the 15-day treatment period but the improvement was much faster and strong in the TP treated group with statistically significant differences vs CP from day-7 onwards.
Difficulty while swallowing is an indication of inflammation and pain, a very common pharyngitis symptom in children. Efficacy results in figure 2 show that at baseline (before 1st treatment), the mean score was slightly low in CP vs TP (5.2 and 6.4/10). Regular throat surface cleaning with saline solution was found to be highly effective in minimizing difficulties while swallowing as a reduction of 5%, 15%, 32%, and 53% was observed on days 1 (2h), 3, 7, and 15, respectively. This reduction was remarkably good in the TP group with a decrease of 15%, 51%, 82% and 96% on days 1 (2h), 3, 7, and 15, respectively (p<0.05 vs CP from day 7 onwards).
Effect on swollen throat
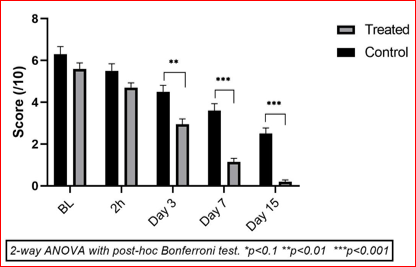
In figure3, the scores were identical in both groups on the 1st day of treatment (BL and 2h post-treatment) but decreased strongly in the TP (n=20, gray bars) vs CP (black bars, n=10) groups from day-3 onwards. Swallowing difficulties eased progressively during the 15-day treatment period but the improvement was much faster and strong in the TP treated group with statistically significant differences vs CP from day-7 onwards.
Results in figure 3 show a slight reduction of swollen throat symptom in both groups, 2 hours after first treatment on day 1 (-16.19% in TP vs -11.42% in CP). Compared to BL values, the mean decrease in throat swelling was fast in both the groups but the reduction was much stronger in the TP group. Some throat swelling was still present in CP group on day 15 but all the patients in the TP group were totally recovered. In CP group, throat swelling was reduced by day 51.42% on day 7 and 66.66% on day 15, compared to baseline. In TP group, the reduction was as high as 53.33% on day 3, 77.14% on day 7, and 97.14% on day 15. The decrease was statistically significant in TP vs CP from day 7 onwards (p<0.001).
Effect on throat irritation
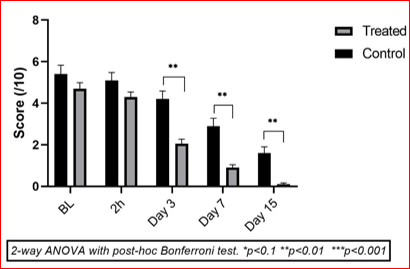
In figure 4, the mean irritation scores started decreasing progressively but the reduction was much faster in TP compared to BL values. Compared to CP, the decrease in TP was statistically significant on day-3 (p<0.01) up to the day-15 (p<0.001).
The mean score of throat irritation started decreasing in both groups 2h after the start of treatment compared to the BL values as seen in figure 4 (-14.28% in CP vs -16.07% in TP). Compared to CP, improvement was much faster in the TP group on day 3 (-32.14% in CP vs -47.32% in TP, p<0.01 vs CP) with further reductions on day 7 (-48.21% CP vs -79.46% TP, p<0.001 vs CP) and day 15 (-67.85% CP vs -96.42% TP, p<0.001 vs CP). The inhibition of throat irritation corresponds to the reduction in throat swelling notices during the same period.
Effect on throat redness (inflammation)

In figure 5, Inflammation started reducing progressively during the treatment period in both groups, but the reduction was much faster in the TP group. Compared to CP, the decrease in TP was statistically significant from day-3 onwards (p<0.01 vs CP from day-3 onwards).
Throat redness is an indication of inflammatory pharyngitis. As shown in figure 5, compared to BL, there were no differences between the 2 groups 2h post first treatment (mean -9.09% CP vs -13.63% TP) but this reduction was much faster and stronger in TP group. Compared to baseline, this decrease was 27.27%, 43.63%, 65.45% in CP vs 56.36%, 84.54%, 99.09% in TP group, on day 3, 7 and 15. The difference was statistically significant (p<0.01) vs CP from day 3 onwards.
Effect on whitish deposit on throat
In figure 6, both saline solution and test product help reducing bacterial deposits during the entire treatment period compared to BL values, but this reduction is much faster in the TP group. The TP vs CP throat surface bacterial growth difference is statistically significant from day-3 onwards (p<0.01 vs CP from day-3 onwards).
Figure 6 shows that here was no significant change in mean scores for the presence of whitish bacterial deposits on the throat surface compared to BL, in both groups on the first day of treatment. From day 3, the results show a sharp fall of symptom score in TP group (-56.38%, p<0.01 vs CP from day 3 onwards) with further reduction on day 7 (-80.85%) and day 15 (-97.87%). In CP group, bacterial growth was also reduced with time indicating a mean decrease of 25.53% on day-3), 53.19% on day-7, and 80.85% on day day-15.
Throat swab analyses
At the start of the study, 9/10 (90%) children in the CP group and 16/20 (80%) in the TP group had a positive throat swab for the presence of bacteria. At the end of the study, only 2/10 (20%) children in the CP group and 3/20 (15%) in the TP group were positive, showing that the bacterial contamination on the throat had sharply decreased in both groups but this decrease was stronger in the TP group.
Use of antibiotics
In the CP saline treated group, 40% children (4/10) required antibiotic therapy for a mean period of 6.3 days compared to only 15% (3/20) in the TP group for a mean period of 5.3 days.
Adverse events
No drug related adverse events were recorded in either group throughout the study.
Overall product assessment
Both products were individually marked by patients and investigators as excellent, very good, good, or fair. The corresponding scores for CP and TP groups were 0%,10%, 65%, 25% for CP and 72%, 25%, 2.5% and 0% for TP group indicating that the test product efficacy was highly appreciated by the users.
Pharyngitis is one of the most common upper respiratory tract (URT) infections in children and the incidence is nearly 3-times less common in adults than in children. Infection transmission rate is nearly 50% [18].Even though the origin of pharyngitis in children is mostly viral, secondary bacterial infection is the main cause of infection, tissue destruction, and pharyngitis symptoms [4]. Group A beta-hemolytic streptococcus (GAS) is considered the most pathogenic microorganism in children pharyngitis and represents 20-30% sore throat medical visits [19].
If left untreated, it may cause post streptococcal glomerulonephritis and acute rheumatic fever (ARF) that is currently uncommon in most developed countries, but it remains the leading cause of acquired heart disease, rheumatic mitral stenosis in developing and low-income group countries [20-22]. Antibiotics and anti-inflammatory drugs always constitute first-line of treatments but increasing microbial resistance to antibiotics [23], GAS is becoming a major health threat to children, even in developed countries [24,25].
If the disease cause is not suppressed within 3-5 initial days, multiple proinflammatory cytokines continue releasing and accumulating on the throat surface which further interfere with the tissue repair process and minimize natural defenses. The cytokines are released on the mucosal surface, but they easily enter systemic circulation through the broken mucosa barrier. Significantly higher inflammatory cytokine levels (TNF-α >1pg/ml,IL-6 >7pg/ml) were detected in most of the pharyngitis patients as opposed to healthy controls. Clinical parameters of infection are also significantly correlated with high levels of inflammatory cytokines [26-28].
This indicates that although pharyngitis is a common disease in children, the upper respiratory tract (URT) presents a complex physiopathology involving millions of newly generated virus particles, bacteria, microbial degradation products, cellular debris, dead cells, multiple proinflammatory and anti-inflammatory cytokines and other proteins on the infected throat surface. These substances continue damaging URT mucosa, causing pain, irritation, itching, inflammation and poor quality of life. This complex physio-pathological chain of events originated because initially a pathogen has killed a cell and caused a cellular damage! Therefore, an effective treatment should first clean the throat surface contaminants to create an ideal environment for rapid healing. Regenerating cells to reconstitute an intact URT cellular mucosa requires a multi-target approach to clean the URT surface of contaminants using a non-chemical and safe mechanism. If contaminants are cleaned and URT mucosa barrier is re-established, disease symptoms should disappear rapidly.
Unfortunately, almost all currently available and commonly used treatments are mono-target, symptomatic, and contain chemicals which are not cell friendly. Pain killers and NSAIDs, such as paracetamol and ibuprofen, help reduce pain and inflammation; anaesthetics such as topical lidocaine reduces only pain sensation; antibiotics like penicillin or amoxicillin minimize bacterial contamination, but these drugs are not totally safe, especially if given too frequently to children. Paracetamol ingestion in very young children increases the probability of hepatotoxicity [29,30] ibuprofen can damage to the epithelium and the micro-vessels of the gastrointestinal system, vomiting and in extreme cases kidney damage [31]corticosteroid therapy may lead to increased appetite & weight gain, fluid retention, and gastrointestinal disorders [32] ; while the use of antibiotics is not always justified or appropriate and may lead to bacterial resistance, which has become a global health threat and economic burden [33]. Antibiotic-resistant bacteria is identified as an increasing issue responsible for high rate of neonate mortality in South East Asian countries [34,35] and over 99 000 deaths in US [36] Above 700,000 deaths per year worldwide are due to antimicrobial resistance and these figures are increasing each year [37].
Therefore, our aim was to find a simple, non-chemical, mechanical and safe mechanism, which can instantly clean and continue cleaning, all the free-floating contaminants from the throat surface. Glycerol is nearly 18 times more osmotic than sea water yet poorly irritant and cell friendly. We rendered glycerol filmogen by binding and stabilizing glycerol molecules with specific polymeric structures having affinity for glycerol. Filmogen glycerol is stable for 4-6h and ensures a long-lasting throat cleaning process. As any osmotic liquid attracts surrounding hypotonic liquid, the out coming hypotonic liquid from the throat surface generates a strong liquid flow which detaches and drains surface contaminants, including pro-inflammatory cytokines. To further improve glycerol stability and to disactivate incoming cytokines, we employed dual-acting polymers, capable of trapping glycerol molecules as well as specific cytokines [38]. The results of the observational study surprisingly show that cleaning the throat surface regularly with saline solution in children, is relatively effective in suppressing symptomatic manifestation of pharyngitis. Unfortunately, 4 to 6 salt-water throat gargles per day is difficult for children. Therefore, just spraying an osmotic yet non-irritant and stable solution on children’s throat surface to get rid of pharyngitis within 2-3 days seems an excellent treatment. Moreover, this product acts nearly instantly as a mechanical antibacterial, anti-inflammatory, analgesic, and totally safe device.
Detaching and draining throat surface adhered bacteria, minimizing inflammation, and keeping the throat surface clean without employing any cytotoxic substance, solely through a simple, safe and instant mechanical device, represents a major advancement to treat one of the most common diseases in children.
ELISA Enzyme-Linked Immuno-Sorbent Assay; NaCl Sodium chlorine; IL Interleukin; BCOP Bovine Corneal Opacity Test; TP Test Product; CP Comparator Product; BL Baseline; URT Upper Respiratory Tract.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
The data presented in this study are available on request from the corresponding author.
The authors declare no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
